
What Does a Fractional VP of Real Estate Do?
Real estate is too consequential to improvise and too intermittent to staff full-time. Here is what a fractional VP of real estate owns for a healthcare operator, how the seat differs from a broker or a consultant, and when a founder or operating partner should bring one in.
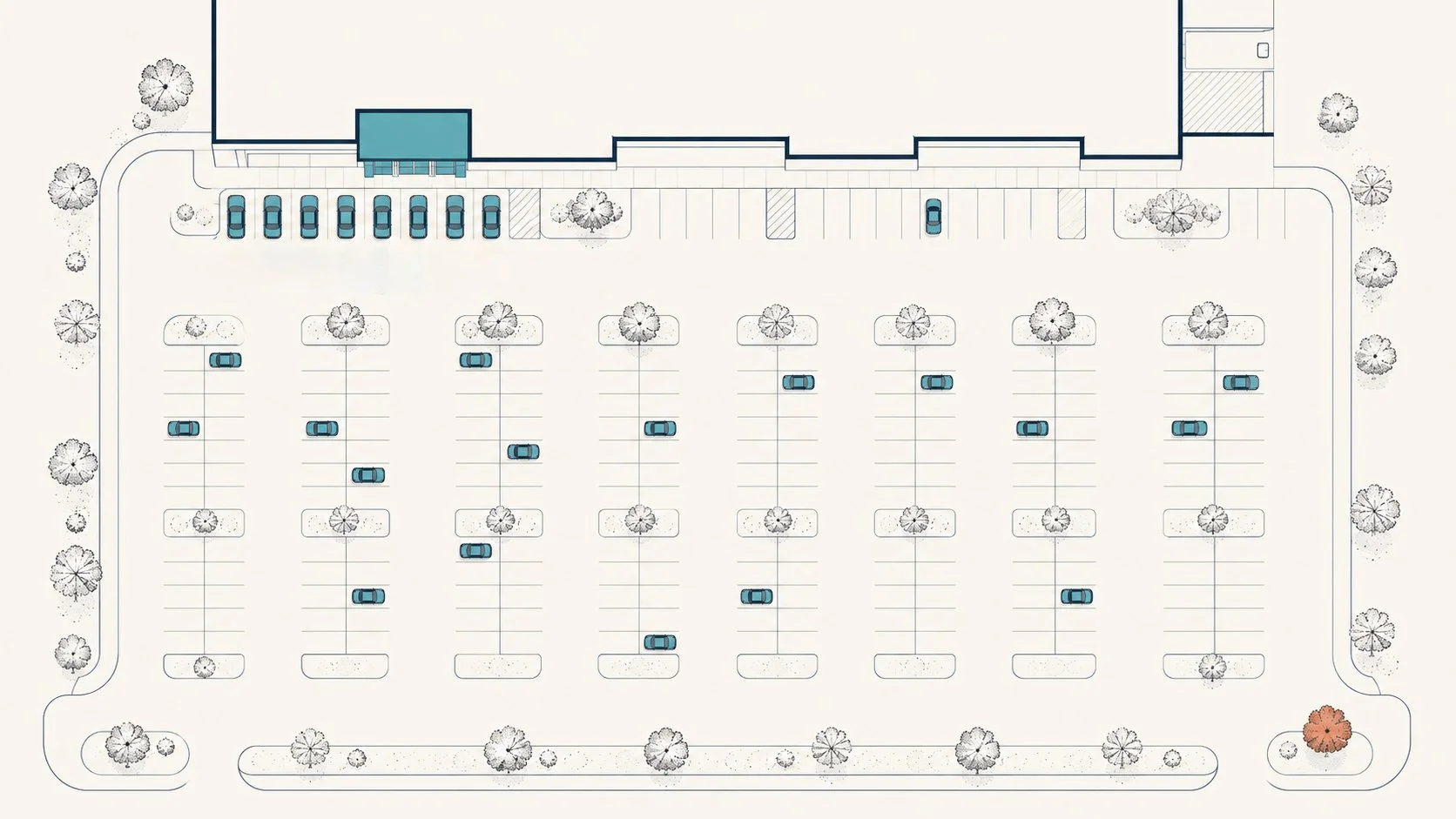
Parking Math
A site checks every box, then you walk the lot at 10 a.m. and there's nowhere to put your patients. Why healthcare parking demand outruns the retail a building was striped for, and how to size it from your care model before you sign.

You Have the CO. You Still Can't Bill.
The build is done, the CO is on the wall, payroll has started — and your first insurance payment is still months away. The licensing, enrollment, and credentialing gauntlet between opening day and your first dollar, and how to compress it.

AI Makes Clients Smarter. Here's the Context It's Still Missing.
A client's AI site analysis trashed the site we were pursuing and praised the one we passed on. Then we gave it the drive-time data and lease economics, and it flipped. Where AI helps, where it goes wrong without your context, and why a human in the loop still makes the call.
The TI Allowance Fine Print: How the Money Moves
The LOI says $340,000 in TI. The lease pages behind it decide whether you collect it. How the money moves — draw packages, deductions, amortized TI — and the five clauses to negotiate before you sign.

Your Patients Are Everywhere. Your First Clinic Can't Be.
Your panel is spread across thirty states. Your first clinic serves a 25-minute drive radius. The patient heat map will point you to the wrong city — here are the four filters that find the right one.
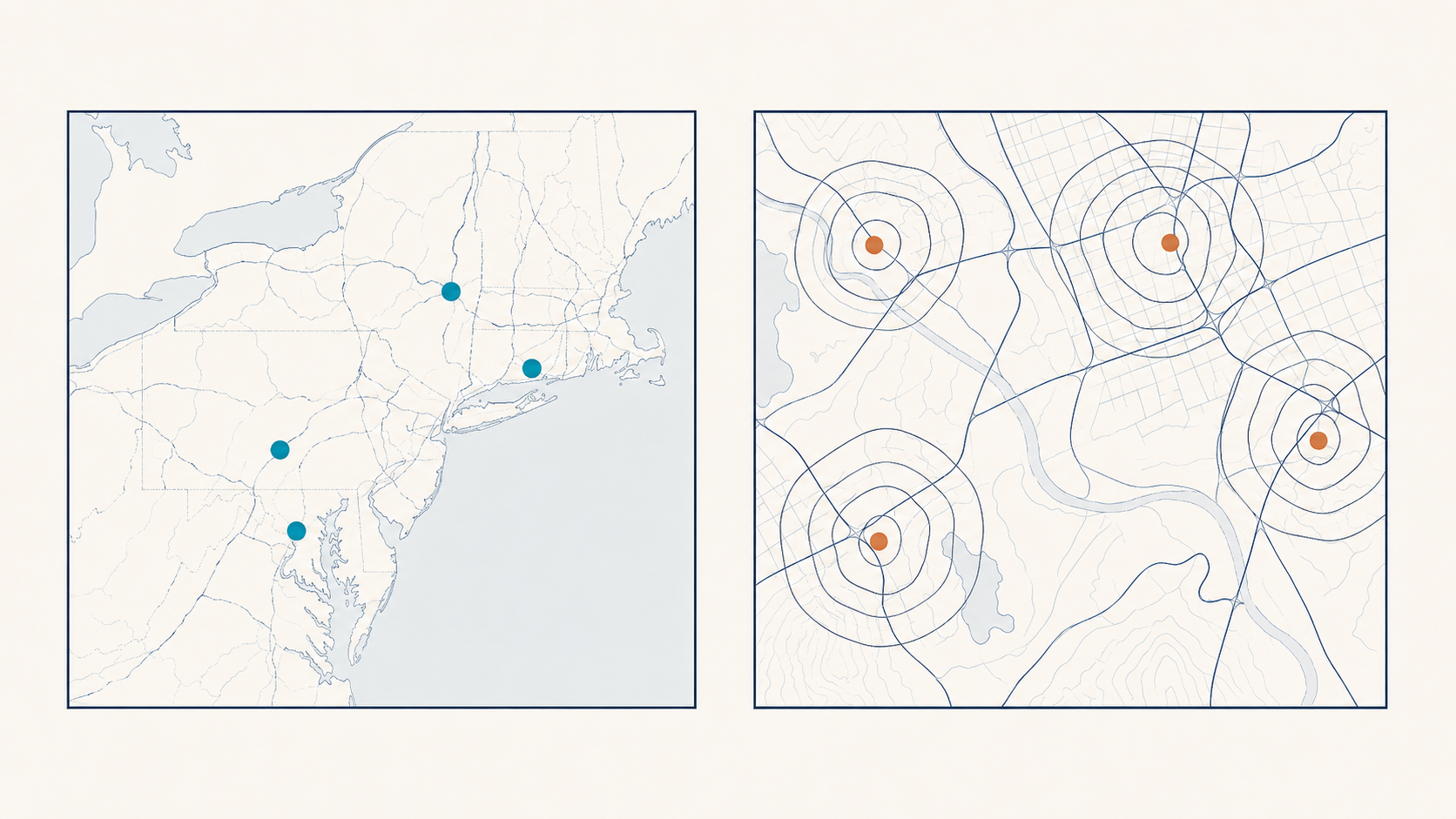
Sites 3 Through 6: One Deep Market or Five Shallow Ones?
Sites 3 through 6 decide whether your clinics compound or just accumulate. Density buys float pools, faster builds, and payer leverage. Spread buys the national story. Here's what each costs, and how to choose.

Financing the Footprint: Why Real Estate Strategy Has to Align with Your CFO
Most healthcare founders model dilution during fundraising but ignore how lease structure and build-out financing quietly increase cost of capital and suppress valuation.

The Fourth User: Designing for the People Who Come With the Patient
Clinics are programmed for three users: patient, provider, staff. The companion who carries the visit home never makes the program. Designing for the fourth user, in the space you already have.

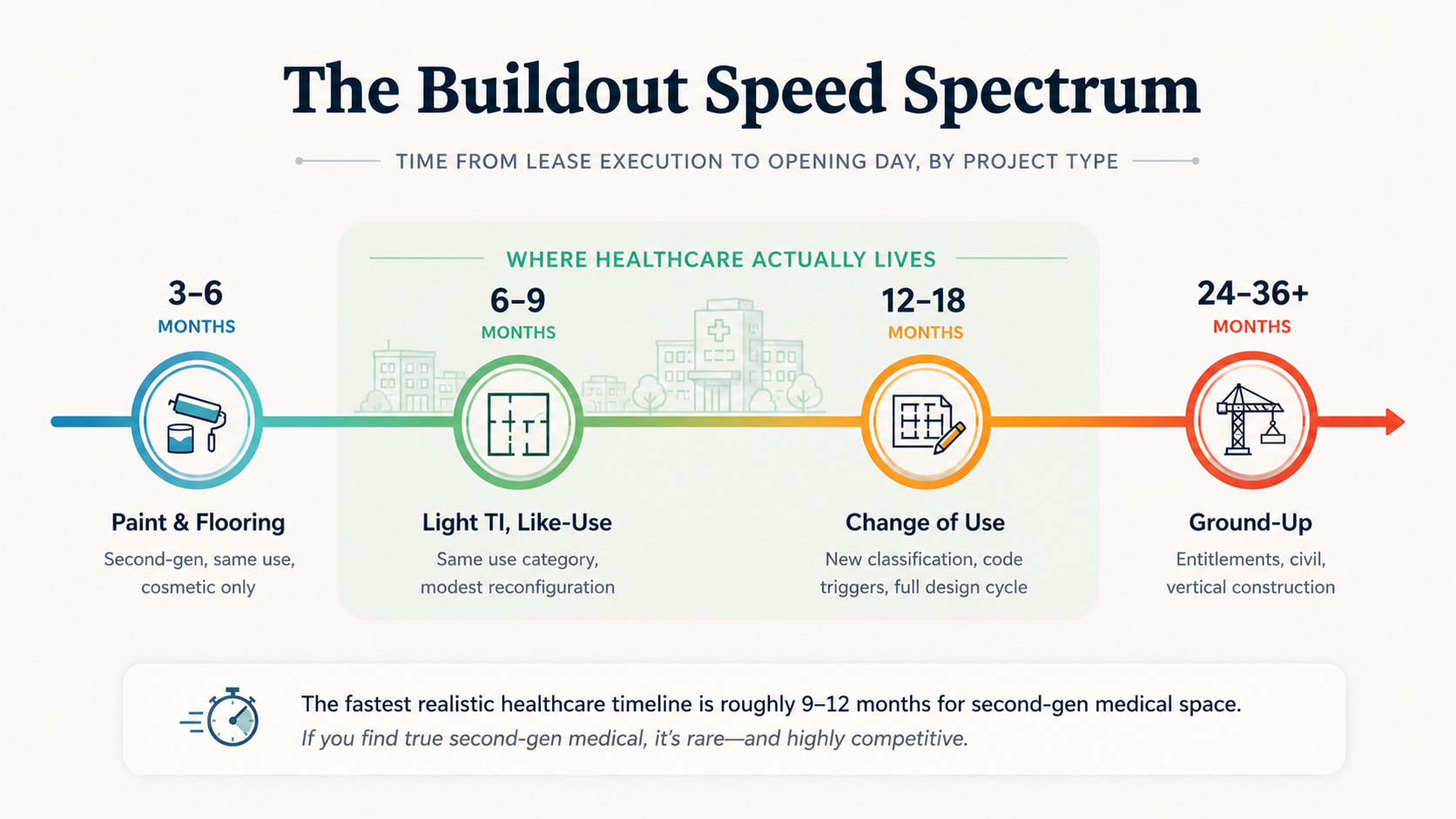
Why Most Healthcare Founders Underestimate Their Clinic Launch Timeline
Most founders think a new clinic is a 6-9 month project. This guide reveals why that thinking is a dangerous trap and what the true timeline looks like.

Construction Is Done. Why You Still Can't Open.
Construction can be finished and your clinic still can't open. The last 2% of a healthcare build runs on inspections and approvals you don’t control. Here's how the inspection-to-CO gauntlet actually works, and how to get ahead of it before your opening date slips.

Your Virtual Model Isn't a Blueprint for Your Physical One
You built a virtual practice and it's working. Now you're adding physical. The operating playbook, the team, the unit economics, the patient acquisition assumptions don’t transfer cleanly. Here's what shows up the day you sign a lease, and what your team has never had to do.
What Physical Care Actually Buys You in a Virtual-First World
Virtual care commodified the easy convenience. What it didn't commodify is the kind of convenience that matters when a patient has real care needs. A reframe on what physical real estate is actually for now, and the contrarian view on what makes it work.

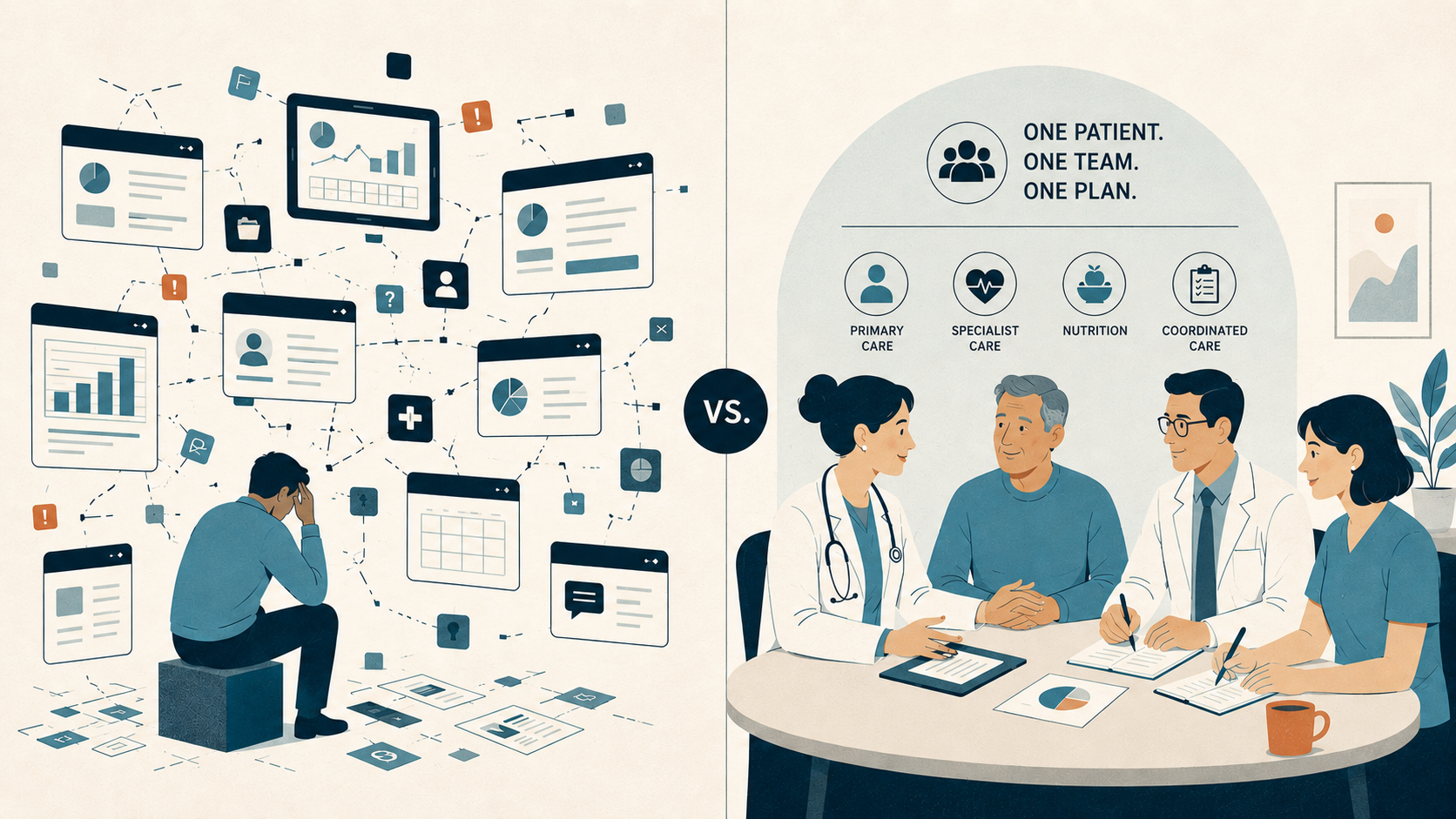
The Coordination System: Who You Actually Need to Build Your First Clinic, and When
A first clinic is four phases, each with specialists who add the most value at specific moments. The seams between them are where 25% of timeline and budget disappear. A phase-by-phase map of who you actually need, when.

Ground-Up Pad or Medtail Lease: The Decision You Make Before Site Selection
An inline medtail suite and a ground-up pad on the same corridor. Both look right on a map. Here's how to run your care model, your capital, and your multi-site plan through the structure before you sign the LOI.
If You Want to Open in 2028, Start Now: The Flexibility–Speed Tradeoff in Healthcare Real Estate
If you want to open a healthcare facility on January 1, 2028, the calendar math says now is the time to start. Here's the flexibility–speed tradeoff.

The Landlord's Math: What Private Building Owners Actually Want From Healthcare Tenants
The private landlord who owns a single freestanding building looks at your deal differently. Owned for 30 years, no debt. They want one thing: a tenant who shows up, pays rent, and doesn't call with problems. Here's their math — and how to negotiate from it.

The First 90 Days: Why Healthcare Handoff Is the Most Fragile Phase
The first 90 days after CO isn't a victory lap — it's a stabilization phase where warranty gaps, workflow friction, and handoff failures get expensive.

Finding Bridge Space When Your Waitlist Is 60 Days Out
Your waitlist is 60 days out and you need exam rooms now. But in tight suburban markets, "move-in ready" clinical space doesn't exist. All three paths have hidden costs—and desperation costs even more than speed.

The Second Site Paradox: Why 1 + 1 Equals 0.5 in Clinic Growth
Site #2 is where healthcare founders learn whether they built a real system or just survived Site #1 through brute force. Here’s why expansion often slows momentum instead of compounding it.