Most healthcare founders approach a new clinic launch as a linear checklist: Find a location. Sign a lease. Build it out. Open the doors.
On paper, it looks like a straight line. In reality, it's a chaotic web of interdependencies. You find a "perfect" site, but the electrical capacity is $200K short of what your imaging tech needs. You sign a lease, but a plan checker's backlog turns a 60-day permit into a 6-month burn on your capital.
These aren't just "project delays." They are System Failures.
If you want to scale a healthcare brand without bleeding cash, you have to stop looking at Real Estate as a series of transactions and start looking at it as The Clinical Engine.
The Shift: From Checklist to Systems Thinking
In my work with scaling healthcare startups, I've realized that the most successful expansions aren't the ones with the biggest budgets—they're the ones with the best System Architecture.
Borrowing from the principles of Systems Thinking pioneered by Donella Meadows in her seminal work Thinking in Systems: A Primer, we can view a clinic launch as a nested hierarchy of sub-systems. Meadows taught us that "a system is more than the sum of its parts—it is the product of their interactions." When these systems are out of sync, the "Engine" stalls. When they're orchestrated properly, you move from chaos to predictable execution.
The diagram below shows the complete Clinical Engine with its six core systems. But before we zoom out to see the whole system, let's understand each component:
1 The Strategy System (The Input)
Every engine needs fuel and a map. In healthcare real estate, this is your Clinical Program.
The System Error: Founders often look for space before they've "coded" their requirements.
The Result: You end up with a "Stock" (the building) that can't support the "Flow" (patient volume/equipment needs), leading to expensive retrofits mid-construction.
2 The Acquisition System (Risk Transfer)
This is about engineering the deal to ensure the "Hardware" (building) and "Operating Partner" (landlord) can support your clinical code.
The System Error: Signing an LOI based on the landlord's "Marketing Flyer" without verifying actual utility capacities.
The Result: You inherit a six-figure infrastructure debt before construction begins. The flyer says "400 Amp Service" but only 200 Amps are actually available to your suite. In systems terms, you've bought the wrong constraints.
3 The Physical Integration System (The Hardware)
This is where Construction, IT, Interior Design, and FF&E collide.
The System Error: Managing these as silos.
The Result: A "System Crash" in the final 10%. The furniture arrives, but the floor-power isn't there. The medical gas is installed, but the wall-blocking is missing. Every "small" oversight here creates a massive delay in your Revenue Generation.
4 The Regulatory System (The Bottleneck)
The local jurisdiction is the "Governor" on your engine's speed.
The System Error: Treating the permit desk as a black box.
The Result: You fall into an Oscillation Loop—submitting plans, waiting 30 days, getting "corrections," and repeating. This is where most healthcare startups lose their Series A momentum.
5 The Execution & Logistics System (The Synchronization Layer)
This is where procurement timelines, construction milestones, staffing ramp-up, and operational readiness must converge.
The System Error: Treating FF&E delivery, team training, and facility completion as independent workstreams.
The Result: Equipment arrives but sits in a warehouse because the site isn't ready. Or the site is ready but your clinical team isn't hired yet. Or both are ready but your IT infrastructure isn't configured. These Synchronization Failures extend your "Dark Period"—paying rent with no revenue.
6 The Activation System (Revenue Ignition)
This is the transition from "Construction Complete" to "Revenue Flowing"—and it's where most startups lose weeks of cash flow.
The System Error: Treating the Certificate of Occupancy as the finish line instead of a trigger point.
The Result: You get your CO but can't see patients because State Licensing isn't complete, payer credentialing is pending, or your staff isn't fully onboarded. The revenue engine sits idle while fixed costs accumulate. In systems terms, this is a Critical Path Failure—the longest pole in the tent just got longer.
Visualizing the Machine: The Lifecycle Map
To manage a system, you have to be able to see it. I've mapped out the Healthcare Real Estate Lifecycle not as a timeline, but as a flow of information and capital.
This diagram shows how the six core systems—Strategy, Acquisition, Physical Integration, Regulatory, Execution & Logistics, and Activation—interact as nested feedback loops. Each node represents a decision point. Each arrow represents information flow. The thickness of the connections shows where bottlenecks typically form.
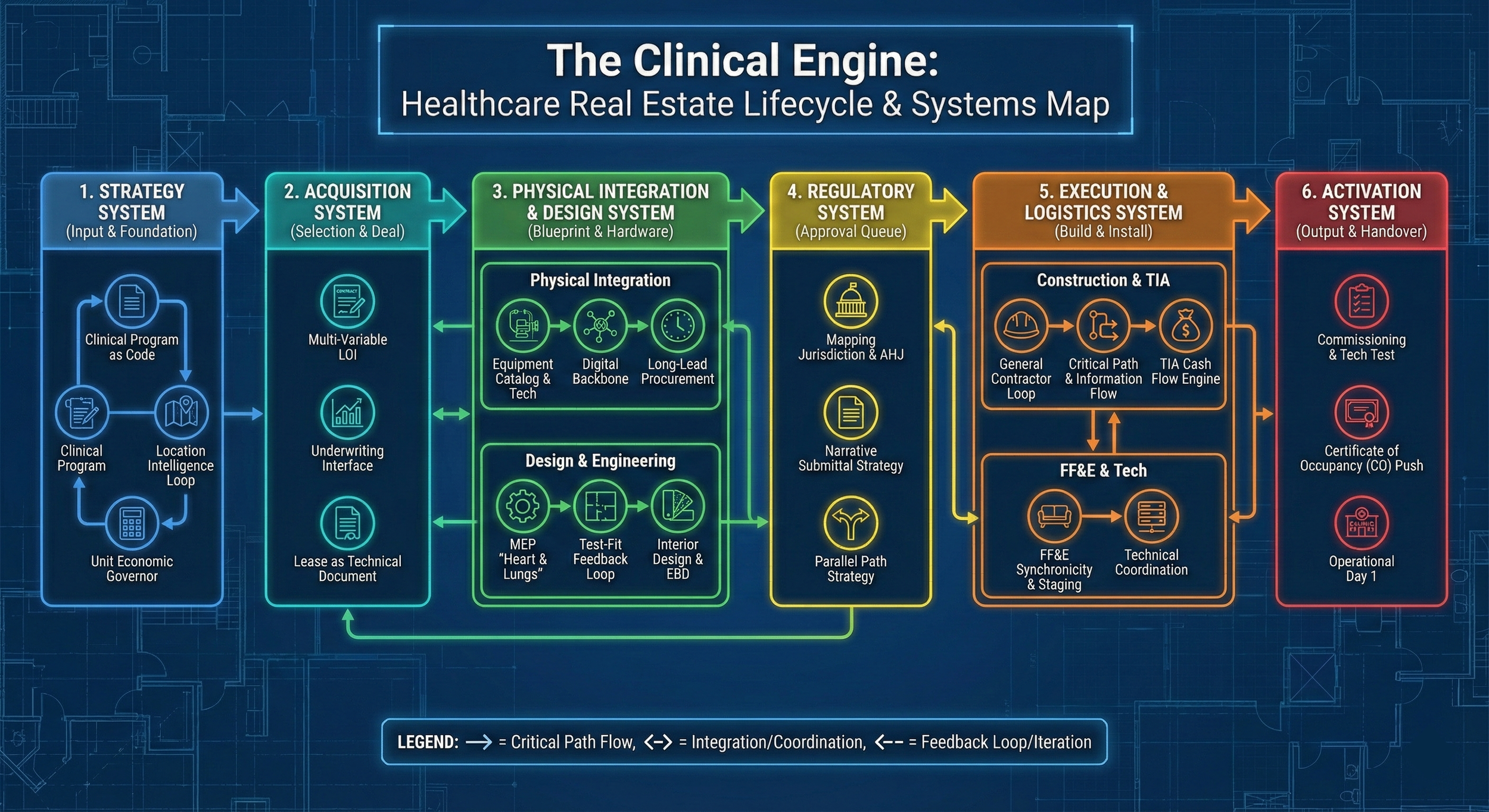
The Clinical Engine: A systems view of healthcare real estate as interconnected flows, not linear steps
Notice how the diagram reveals what a linear checklist hides: Every decision you make in the Strategy System creates constraints (or opportunities) in the Acquisition System. Every deal structure in the Acquisition System impacts what's possible in the Physical Integration System. Every delay in the Regulatory System compresses timelines in Physical Integration. Every integration failure creates chaos in the Execution & Logistics System. And every logistics breakdown extends the gap between your CO and your first patient—the Activation System.
This is why treating real estate as a "checklist" fails. As Meadows writes: "The behavior of a system cannot be known just by knowing the elements of which the system is made." The system has memory. It has feedback loops. And it punishes you for treating interconnected parts as if they were independent. One broken link doesn't just delay that phase—it cascades through every downstream system.
Managing the Flow: Why This Matters for Founders
Time is the only resource you can't recover. In a high-barrier market like California, the difference between a "Systematized" launch and a "Checklist" launch is often 4–6 months of burn.
By professionalizing your real estate "Strike Team" and viewing the build-out as an integrated engine:
Eliminate the Startup Learning Curve
You aren't learning how a parking variance works on your own dime.
Establish Execution Certainty
Landlords sense your readiness and offer better terms (TIA, Rent Abatement).
Build a Scalable Template
Once the "Engine" is built for Site #1, Site #2 through #10 become a matter of replication, not reinvention.
What's Next: Breaking Down the Clinical Engine
Over the coming weeks, I'll be breaking down each component of the Clinical Engine in detail:
- Section 1: The Strategy System — How to "code" your clinical program for maximum ROI and avoid the $200K retrofit
- Section 2: The Acquisition System — Engineering the deal to transfer risk and buy execution certainty, not just cheap rent
- Section 3: The Physical Integration System — Synchronizing Construction, IT, and FF&E on the critical path
- Section 4: The Regulatory System — The micro-politics of the plan review desk and beating the permit bottleneck
- Section 5: The Execution & Logistics System — Coordinating procurement, staffing, and facility readiness
- Section 6: The Activation System — Turning a CO into cash flow without burning weeks of revenue
The goal isn't just to open a clinic. The goal is to build an expansion machine that can out-execute the competition every time.