When a founder asks us "When could we open?" — that's almost always the wrong question. The right one runs in the opposite direction: "If we want to see patients on January 1, 2028, what does our search behavior need to look like right now?"
When you do that math, the answer is rarely what people expect. 2028 is not a comfortable distance away. It is roughly the timeline you'd actually want — assuming nothing major goes sideways. And the more flexible you are willing to be on building, location, rent, and buildout scope, the more of that timeline you keep in your favor.
Healthcare real estate has a flexibility–speed tradeoff at its core. The less flexibility you carry into the search, the more calendar you spend.
The Flexibility–Speed Spectrum
How fast you can open a building is a direct function of how flexible you are willing to be — on location, building type, rent, and buildout scope. The more constraints you carry into the search, the longer the calendar gets.
For non-healthcare uses, the spectrum runs from very fast to very slow:
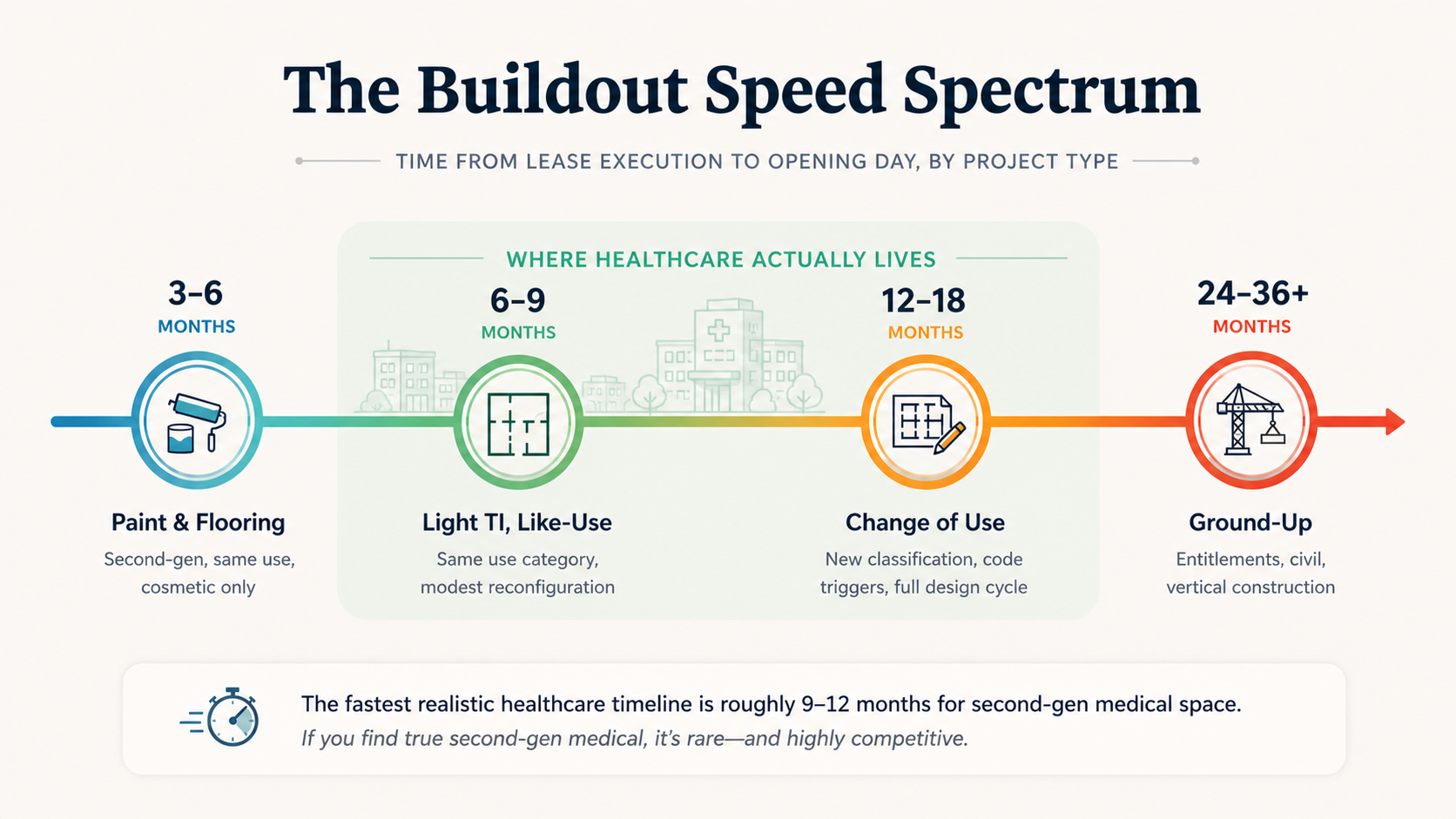
Healthcare almost never lives at the fast end. The medical-grade MEP, infection control, accessibility, and code triggers tend to push what looks like a paint-and-flooring job into change-of-use territory once you scratch the surface. Most healthcare projects sit in the middle band of the spectrum — and the further right you slide, the more runway you need.
The Zoning Trap That Eats 60–90 Days You Didn't Budget
This is the part that's easy to miss until you're already in escrow on a lease.
Medical office is its own use category in nearly every jurisdiction. It is not "office." A building that is zoned and entitled for general office may be a perfectly fine asset, but it is not pre-cleared for medical use, and bridging that gap is not cosmetic. It is regulatory.
What a Change of Use Actually Triggers
When you change the use from general office to medical office, you frequently trigger:
- A change-of-use permit, which is its own review track
- Parking ratio recalculations (medical typically requires more parking per square foot than office)
- Path-of-travel ADA upgrades that can extend beyond your premises into the building common areas and parking lot
- Building classification changes (often from B occupancy to a healthcare or institutional classification) that drive structural, fire, and life-safety requirements upward
- Conditional Use Permit hearings in some jurisdictions, which run on a public-meeting calendar that doesn't care about your funding timeline
Any one of these can absorb 60 to 90 days. Stack two or three of them and you've quietly added a quarter to your timeline before construction starts.
The fastest projects we've worked on weren't the ones that found the cheapest space. They were the ones where the search criteria included "already entitled for medical use" as a non-negotiable — or where the team was willing to walk away from a beautiful space that wasn't. Cheap upfront often costs you the calendar.
Working Backward from January 1, 2028
Pick a target opening date and the math becomes concrete. Here is what a realistic working-backward timeline looks like for a moderately complex healthcare project — change of use, second-generation building, no ground-up construction:
The Calendar, in Reverse
In other words: a project targeting January 1, 2028 should already have a market identified and site search started. If you are just now starting to think about where to expand, to open January 1, 2028 everything that has to go right.
This isn't pessimism. It's calendar arithmetic. Each phase has a floor that is set by people, processes, and reviews you don't control. You can compress some of it through parallel pathing in the regulatory phase and disciplined coordination — but you can't compress all of it, and you can't compress the parts that depend on the city.
The PACE Operators Who Already Understand This
Nowhere is this clearer than PACE.
In California, DHCS paused new PACE organization applications and service-area expansions for existing organizations on November 20, 2025. The pause runs through at least November 19, 2027, and the timeline could extend depending on how DHCS uses the window to revise the application framework.
PACE center development typically runs 24–36 months end-to-end — site search, entitlements, design, construction, licensing, and CMS application. So if you are an operator planning to compete in the post-moratorium window, the math is unforgiving:
The November 2027 reopening is not a starting line. It's a midpoint.
The operators who will be ready to file applications the day the window reopens are the ones who already have sites identified, leases negotiated, design underway, and entitlements running today.
Site search alone for a PACE-suitable building — adequate parking, ADA-friendly access, transportation logistics, the right zoning, the right neighborhood density of eligible seniors — can take six to twelve months on its own.
There are also strategies for advancing a project in parallel with the moratorium while hedging against the risk that the window doesn't reopen on schedule, or that the entry requirements get materially more demanding when it does. Those strategies are project-specific — they depend on your capital structure, your geography, and what posture you want with DHCS — and they're worth a real conversation rather than a public checklist. The operators using them are quietly getting further ahead every month.
This is not a California-only dynamic. PACE is launching in Nevada. We are hearing early signals from other states. Each new market will have its own version of the same compression: a long development timeline meeting a regulatory front door that opens on a specific date. The operators who treat the moratorium as a pause are going to get beaten by the operators who treat it as a runway.
What "Flexibility" Really Buys You
Opening on time has less to do with finding a perfect site than with treating flexibility as a strategic input from day one.
The Constrained Search
"We need 6,500 square feet, on the corner of X and Y, ground floor, with these visibility characteristics, at this rent."
You are essentially waiting for one specific space to come available at the right time, especially in a tight medical office submarket. Hope is not a strategy.
The Flexible Search
"Here are our care-model-driven non-negotiables — zoning, MEP capacity, parking ratio, patient-flow logistics. Here is what we will trade off — exact location, building age, finish quality, rent within a band — to compress the calendar."
You've widened the funnel without compromising what actually matters for care delivery.
We've written before about how care model drives real estate, not the other way around — flexibility is the operational version of that principle.
The tradeoff is real. You may pay slightly more in rent. You may end up in a building you wouldn't have picked if you had two more years. But you open on time, you start generating revenue on schedule, and you don't burn another twelve months of payroll, executive time, and investor patience waiting for a unicorn.
The Search Is the Strategic Act
If there's one thing we want healthcare founders to take from this: the search is not a precursor to your strategy. The search is your strategy. How you scope it, how flexible you make it, how early you start it, and what network you have feeding it deals — those decisions determine whether you open on your timeline or someone else's.
We're Always Tracking Healthcare-Suitable Space
We're not a brokerage, but we keep a strong pulse on the market — talking to healthcare brokers, developers, landlords, and operators across the country. Because we are actively developing PACE centers and clinics, people in our network call us first when something interesting is coming available. We hear about medical-zoned buildings, second-gen medical spaces, and well-located change-of-use candidates before they hit the public market.
If you are thinking seriously about a 2027 or 2028 opening — whether that's a primary care clinic, a specialty practice, or a PACE center in California, Nevada, or any of the markets quietly heating up — we'd like to be in early conversation. Not because we have a deal to sell you today, but because the projects that open on time tend to be the ones where the strategic conversation started a year before anyone thought it needed to.
We'll talk through:
- What your care model actually requires from the building (and what it doesn't)
- Where flexibility on your search criteria buys you the most calendar
- Which markets and submarkets are worth pre-positioning in
- How to hedge timeline risk against regulatory windows like the California PACE moratorium